APOE and the genetic architecture of postoperative delirium
Postoperative delirium is a common and serious complication in older people after major surgery. In a new PLOS Medicine paper led by Richard Armstrong, we investigated whether inherited genetic variation helps explain risk of postoperative delirium, and how that risk relates to broader neurocognitive conditions.
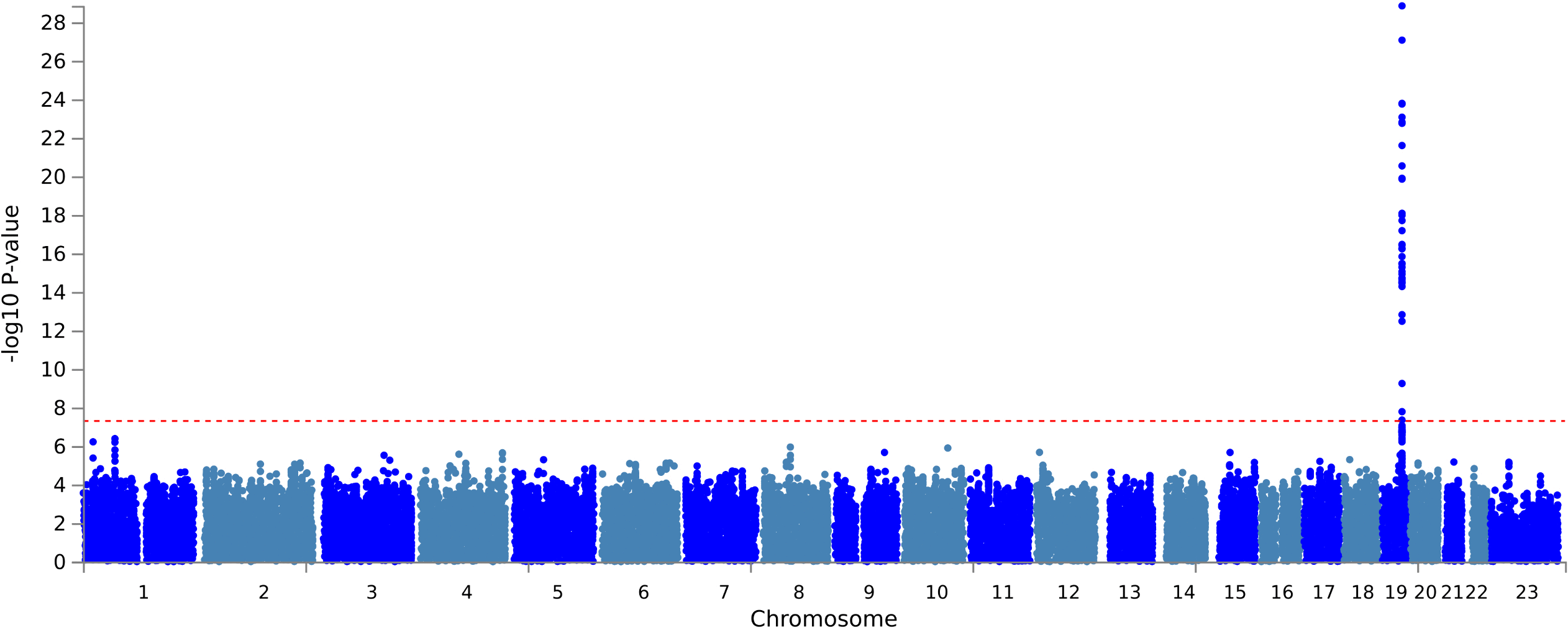
Figure: Manhattan plot from the postoperative delirium GWAS, with the genome-wide significant signal concentrated at the chromosome 19 APOE region. Source: Armstrong et al., PLOS Medicine, 2026, Fig. 2 (CC BY 4.0).
Background
Delirium after surgery is clinically important because it is associated with poorer recovery, longer hospital stays and later cognitive problems. It is also difficult to study genetically: postoperative delirium is an acute event, clinical coding can miss cases, and the number of well-phenotyped cases is much smaller than for many chronic diseases.
This study used UK Biobank linked health records to identify people who had major inpatient surgery and then developed delirium within 30 days. It then compared genetic results for postoperative delirium with delirium of any type and Alzheimer's disease.
What the study did
The primary genome-wide association study included 1,016 postoperative delirium cases and 139,148 controls who had undergone major surgery without a recorded delirium diagnosis in the postoperative window.
The authors then used follow-up analyses to ask whether postoperative delirium shares genetic architecture with:
- all-cause delirium;
- Alzheimer's disease;
- the APOE epsilon 4 allele, an established genetic risk factor for Alzheimer's disease.
What we found
The GWAS identified seven genome-wide significant variants in a chromosome 19 region mapping to APOE, TOMM40, APOC1 and PVRL2. The lead variant was rs429358, one of the variants defining APOE isoforms.
The study also found evidence of shared genetic liability between postoperative delirium and Alzheimer's disease. APOE epsilon 4 showed a dose-response relationship with postoperative delirium risk after adjustment for age and sex: risk was higher for people carrying one copy and higher again for people carrying two copies.
Importantly, some associations remained after excluding people with pre-existing dementia, and after excluding people with subsequent dementia. That does not prove mechanism, but it argues that the signal is not simply a reflection of already diagnosed dementia in the dataset.
Why this matters
These findings support the idea that postoperative delirium may, at least in part, reflect underlying vulnerability in neurocognitive biology. If replicated and extended, genetic information could eventually contribute to preoperative risk stratification or to identifying people who may benefit from closer postoperative follow-up.
There are important caveats. The delirium phenotype relied on clinical coding, which is likely to miss some true cases, and the study had limited power to detect small genetic effects. The findings should therefore be treated as a foundation for further work, not as a clinical genetic test.
Paper
Armstrong RA, Yousefi P, Gibbison B, Khandaker GM, Gaunt TR. The genetic architecture of postoperative delirium after major surgery and its relationship with nonpostoperative neurocognitive conditions: A genome-wide association study. PLOS Medicine (2026) 23(3):e1004963. DOI: 10.1371/journal.pmed.1004963. PubMed: 41770756. Full text: PMC12970968.